

Everybody Loses with Most Favored Nation Reference Pricing. . .Except China.
By Duane Schulthess and Harry P. Bowen
June 23, 2025
Key takeaways
- If MFN were adopted in Medicare and Medicaid, based upon our preliminary estimate, it could lead to 1.3 million fewer jobs over ten years.
- $2.8 trillion in lost earnings over 10 years due to MFN being applied to Medicare, resulting in $700 billion in reduced tax revenue.
- By undermining the U.S. economic environment, MFN risks accelerating the movement of U.S. biopharma research and development to China.
On May 12, 2025, the Trump Administration issued an Executive Order (EO) entitled “Delivering Most-Favored-Nation Prescription Drug Pricing To American Patients”. In it, President Trump acknowledges that Americans pay too much for medicines while other countries don’t pay enough. This imbalance means U.S. patients are subsidizing global drug development, and President Trump wants it to stop.
On the surface, how can one argue? According to a February 2024 report of the Assistant Secretary for Planning and Evaluation (ASPE) of the U.S. Department of Health & Human Services (HHS), “In 2022, U.S. prices across all drugs (brands and generics) were nearly three times as high as prices in 33 OECD comparison countries. For every dollar paid in other countries for drugs, consumers in the U.S. pay $2.78. The gap is widening over time.”
The current administration’s “Most Favored Nation” (MFN) executive order is short on implementation details, punting most of the rule-making to HHS and other government agencies. However, this is not the first time a Trump Administration has tried MFN reference pricing.
During the final days of the previous Trump Administration, the Centers for Medicare & Medicaid Services issued rulemaking for the implementation of MFN in Medicare Part B as a demonstration. It was blocked in federal court by an injunction in response to a complaint filed by the Biotechnology Innovation Organization(BIO), California Life Sciences, and Biocom California, ultimately leading to the rule being rescinded by CMS in 2021. However, if we assume that the new MFN is similar to the original filed in 2019, we expect an MFN price to be taken from the lowest found in a cohort of countries that are within 60% of U.S. GDP per capita, using the pricing taken from the February 2024 RAND report for the Assistant Secretary for Planning and Evaluation (ASPE) U.S. Department of Health & Human Services.[1]
Vital Transformation (VT) is in the process of calculating MFN’s impacts upon the global biopharma ecosystem if adopted wholesale into U.S. Medicare Parts B and D. The release of that report is imminent. However, VT recently completed an assessment of an implementation of MFN upon the top 50 drugs by expenditure in Medicaid using data from the report referenced above and the CMS dashboard, as was originally reported to Inside Health Policy to be the scope of MFN. VT’s impact assessment of MFN for Medicaid (as well as the 340B program), can be found here. Findings show that if MFN pricing were adopted for the top 50 drugs in Medicaid, it would lead to over 440,000 fewer jobs in the United States and a loss of over $356 billion in taxes paid over 10 years.
A recent report by Berkeley Research Group finds that the net costs of the combined programs of Medicare Parts B & D are roughly two times larger than the combined programs of Medicaid and 340B. If we assume that the impact of reduced revenues due to MFN for the top 50 drugs by expenditure in Medicare is both linear and roughly similar to that for Medicaid & 340B, we can do a bit of ‘back of the envelope’ math and scale-up our now released Medicaid impact assessment.[2]
U.S. Jobs

Figure 1 Extrapolated MFN Medicaid analysis for U.S. jobs lost scaled to Medicare.
Harnessing data obtained from the U.S. Bureau of Economic Analysis and applying MFN prices in Medicare to the top 50 drugs by expenditure, we estimate that the U.S. will lose 869,000 jobs over the ten-year period of 2025 – 2034. 185,000 of these jobs are lost in direct biopharmaceutical employment, and 683,000 are lost in indirect support of the sector.
At the U.S. state level, California is most impacted, with 94,000 jobs lost. New York loses nearly 60,000 jobs, followed by Texas, Ohio, and Pennsylvania, cumulatively losing 149,000 jobs.
Wages and Taxes
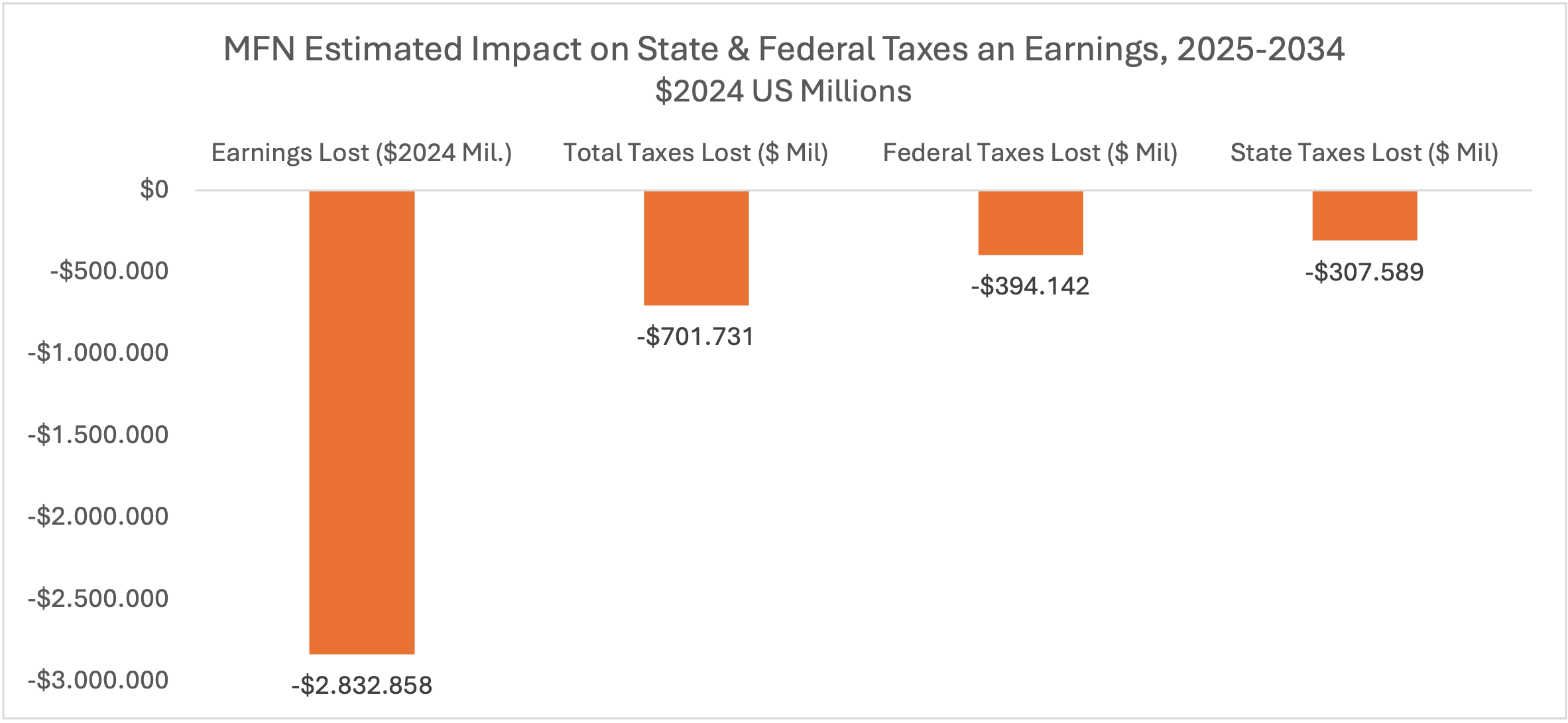
Figure 2 Extrapolated U.S. Wage and Tax results of MFN Medicaid analysis scaled to Medicare.
According to the trade publication Biospace, “As of 2023, the average overall salary for U.S. life science professionals is $142,885,” implying that those directly employed in the biopharma sector who will be impacted by MFN are highly paid and skilled.
We estimate that applying MFN to the top fifty drugs by expenditure in Medicare Parts B & D would lead to an annual loss of direct and indirect wages of $283 billion, roughly 3% of total projected annual wages paid according to data from the U.S. Bureau of Labor Statistics. We further estimate that these lost wages will result in $70 billion in lost taxes annually over 10 years, with roughly 60% of those tax losses being at the federal level.
Why Can’t Companies Simply Raise Their Prices in Other Countries?
Many other countries in Europe and elsewhere have only public health insurance. Governments in these other countries set drug prices and choose which drugs are reimbursed by public health insurance. Many governments choose to spend less on innovative medicines in favor of other fiscal priorities. Patients in these countries typically don’t have the option of acquiring private health insurance to cover the medicines not reimbursed by the public health insurance.
Pinning an MFN negotiation on an individual company risks forcing governments to use all available leverage. Nearly all foreign governments maintain powers, known as compulsory licensing, to override patents on ambiguous grounds, including pricing, to enable local manufacturing. Most recently, the United Kingdom and the Netherlands have threatened to issue compulsory licenses during innovator price negotiations. Companies have limited negotiating leverage under these circumstances. Further, walking away from the negotiation and deciding not to launch a product could be cited as grounds for a government to issue a compulsory license.
MFN ignores the simple reality that forcing a drug’s price to be far below its free market price will inevitably lead to reduced access due to rationing and shortages. According to a joint report published by the French Pharmaceutical Industry and the French Government, delays in access to medicines in France, “are among the longest in Europe . . . with an average of 530 days between market authorisation and [access].”
In fact, most EU countries severely restrict access to medicines approved by the European Medicines Agency (EMA). A report from the Swedish Institute for Health Economics states that “Malta, Estonia, Slovakia, and Romania reimbursed fewer than 20% of new medicines and the average time to reimbursement was close to 900 days in Latvia and Lithuania, leading to stark inequalities in patient access to new treatments.”
Whilst popular rhetorically, it is highly unlikely that U.S. consumers and practitioners will accept an MFN policy that creates shortages and access restrictions. Yet, enforced prices below open market prices inevitably lead to rationing.
Forcing U.S. Innovation to China
VT’s recent peer-reviewed study on the impact of the Inflation Reduction Act (IRA) shows that venture capitalists (VCs) are already avoiding investing in medicines targeting the Medicare-aged population. These impacts are also now becoming manifest as a lack of biopharma company creation. Data extracted from Pitchbook in May of 2025 shows a 50% drop in company start-ups since IRA’s introduction. The largest drops are in California and Massachusetts.

Figure 3 Data extracted from Pitchbook May 2025, company start-ups by creation date.
MFN has the potential to exacerbate an already profoundly negative economic environment for U.S. biopharma, and to further incentivize a movement of research assets to China. This is the exact opposite outcome from what MFN professes to be its stated goal, namely, an improved situation for U.S. patients and consumers.
According to a May 6, 2025, article by former FDA Director Scott Gottlieb, “Five years ago, U.S. pharmaceutical companies didn’t license any new drugs from China. By 2024, one-third of their new compounds were coming from Chinese biotechnology firms.” Nowhere is this more evident than by observing recent data on the number of FDA-registered clinical trials by Chinese firms, which have increased by nearly four-fold since 2018.

Figure 4 Chinese FDA registered clinical trials by year. Source: Biomedtracker.
The Trump Administration must rethink its approach to MFN. Relying on a company to unilaterally raise its drug prices in foreign markets will be a failure since foreign governments have all the power.
Instead, the U.S. Government must engage directly in drug pricing as part of its strategy of trade negotiations. If not, we’ll see a rapid acceleration in the movement of U.S. Biopharma research and development to China and a gutting of available free cashflow for U.S. based biopharma R&D. Such a shift is not unprecedented, as it is effectively what has transpired since the mid-1980s, with biopharma investment shifting away from Europe and toward the United States due to increasingly stringent EU price controls and related policies compared to in the U.S.
[1] https://www.cms.gov/newsroom/fact-sheets/fact-sheet-most-favored-nation-model-medicare-part-b-drugs-and-biologicals-interim-final-rule
[2] The methodology and assumptions of our MFN Medicaid analysis can be found here: https://vitaltransformation.com/wp-content/uploads/2025/10/MFN-v8_6.23.25-V21jul-2.pdf