Blog: Don’t Believe the Hype – International Reference Pricing Will Cost Far More than 1% of R&D Budgets
By Duane Schulthess – 26 December 2018
“Every government intervention creates unintended consequences, which lead to calls for further government interventions.”
Ludwig von Mises
It’s odd that a city like Brussels managed to carve itself out a niche as one of the major political centres of the world. The medieval site of a notoriously typhus infested bog, one of the main streets in downtown, ‘Rue du Marais’, literally means, “Street of the Swamp” and the name of the city itself comes from the old Flemish word Broekzele, which roughly translates to ‘settlement in the swamp.’ So, when one talks politically of draining the swamp, at least in Brussels, it carries a literal interpretation that is often distant from the current political climate in DC.
What goes without question is that both Brussels and DC are currently heaving under waves of increasing populist threats to drain political swamps. With the Brexit referendum followed by the election of President Trump, we also now have the Yellow Vest protests in France coupled with a letter accusing President Macron of treasonsigned by a dozen French generals and a former Minister of Defense. There is an air of anger against political institutions on both sides of the Atlantic, and increasingly, the heated rhetoric is being pointed at the price of medicines.
For the last 24 months, Brussels has seen an influx of U.S. financing for ‘grass roots’ organisations focused on EU access and reimbursement for medicines. The Open Societies Foundation and the Helmsley Trust amongst others, have poured millions of dollars into extremely well organised campaigns targeting Europe’s reimbursement system for medicines; a key plank in the European Institution’s solidarity charter guaranteeing equal treatment for all within the member states. This went as far as some activists even questioning the need for intellectual property (IP) and private drug development at all. Kayum Ahmed of the Open Societies Foundation in his introduction of a session at European Health Forum Gastein, on October 3rd, 2018, said “Research shows the public institutions fund most of the health and innovation . . .taxpayers are now paying twice.”
It was at this point that Vital Transformation entered the discussion, showing quite conclusively that private funders invested more than 500 times what the EU institutions contributed to biotech innovationthrough their framework programmes. The numbers are so convincing, it is a shame that they even need to be discussed. Sadly, much in the same way that NASA for many years avoided lending its voice to the debate on the ‘faked’ moon landings, innovators must start addressing the increasing falsehoods related to the price of medicines, profits, and the current climate of international innovation.
In reality, it is understandable that US politicians would want to discuss the unequal pricing of medicines globally, as European medicines are subsidised by US tax payers. The current US administration is simply playing the populist ‘Trump’ card to reduce prices in America too.
However, whilst this may be good politics in America, the unintended consequences could be devastating to US innovation and R&D leadership. It is vital to understand the implications of what is, in essence, the establishing of rent controls and price ceilings for medicines in the United States.
What Would Reference Pricing Do?
On October 26, 2018, Alex Azar, the Secretary of the U.S. Department of Health and Human Services gave a presentation at the Brookings Institution. He outlined the administration’s new proposal to lower prices for Medicare Part B drugs through international reference pricing. He said, “The payment model is based on a new report we put out on Thursday which examined the gaps between what we pay and what other countries pay for the 27 highest-cost physician-administered drugs. According to our research, right now Medicare pays 180 percent of what other wealthy countries pay for this set of costly drugs”
On this point, Secretary Azar is 100% correct. The current international reference pricing strategy as announced by Secretary Azar was initially floated in the Council of Economic Advisor’s report in February of 2018, where the need to address the current gap in prices between the United States, Japan, and Europe was outlined.
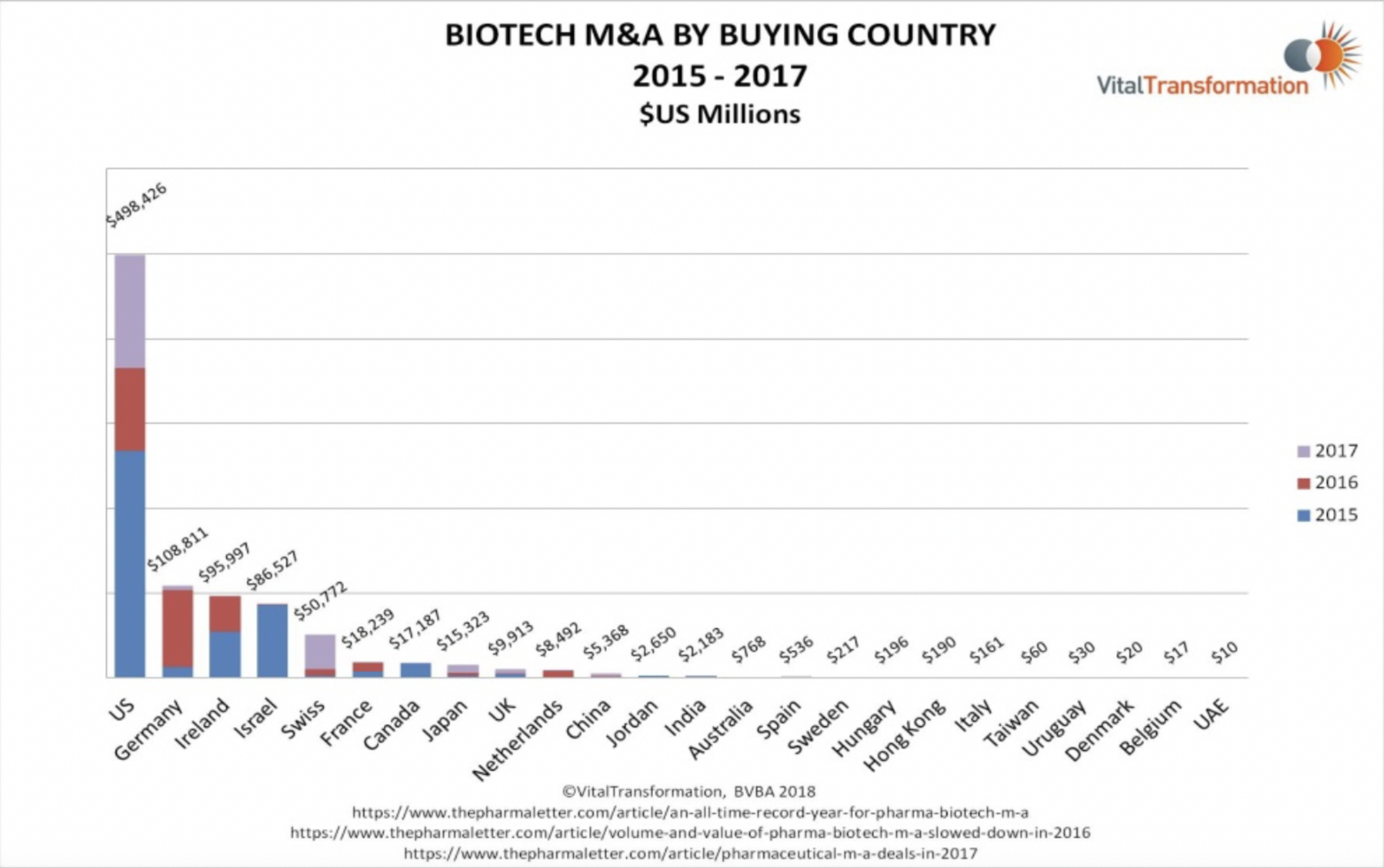
What has not been discussed in the Brookings’ announcement is the role the U.S. currently plays in global innovation and IP. According to our research, 70% of mature global biotech companies are being acquired by the United States. While it is true that prices are higher in the US, the knock-on effect is the US domination of the global landscape in biopharmaceutical development and R&D.
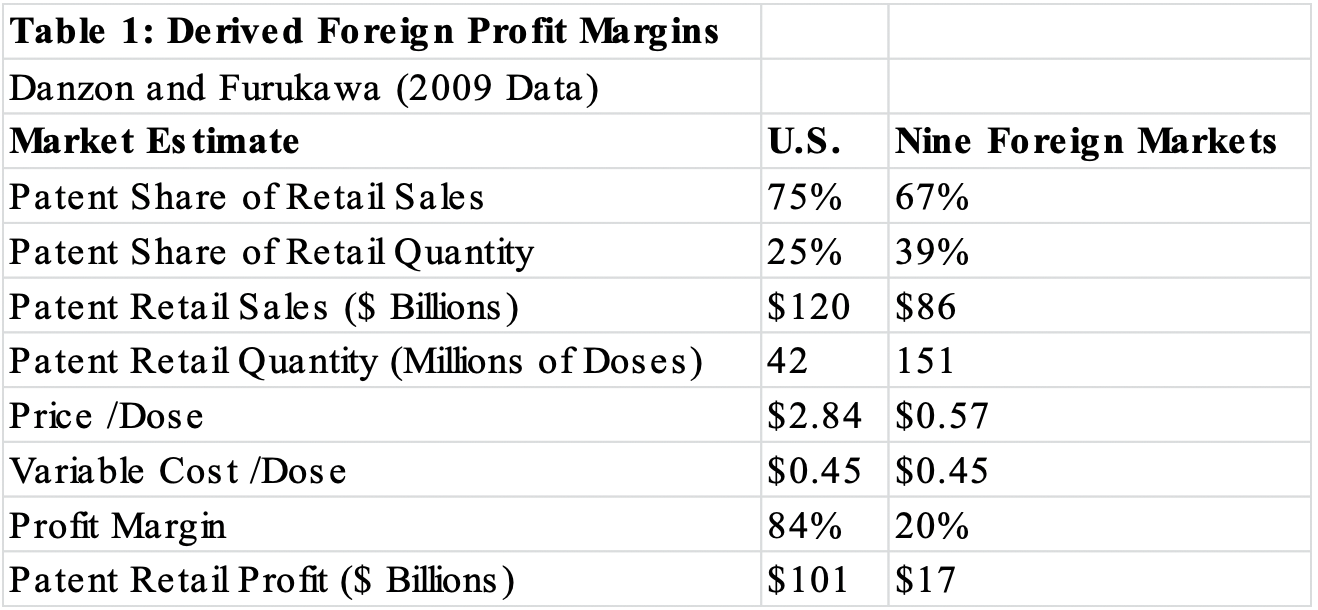 In a recent podcast with Richard Bergström, the former Director General of the EU’s pharmaceutical lobbying organisation EFPIA, he said, “Being in Cambridge, MA, it’s really the capital of the industry. . . It strikes me, the stark contrast between Europe and the US in that sense; all the wealth, the interplay between finance and pharma, is in the US. The money is there, and it’s a real problem for Europe.” This is best demonstrated by data included in the abstract of the Council of Economic Advisors’ Report related to the ability of each region to monetise intellectual property (Table 1).
In a recent podcast with Richard Bergström, the former Director General of the EU’s pharmaceutical lobbying organisation EFPIA, he said, “Being in Cambridge, MA, it’s really the capital of the industry. . . It strikes me, the stark contrast between Europe and the US in that sense; all the wealth, the interplay between finance and pharma, is in the US. The money is there, and it’s a real problem for Europe.” This is best demonstrated by data included in the abstract of the Council of Economic Advisors’ Report related to the ability of each region to monetise intellectual property (Table 1).
According to the researchers Danzon and Furukawa, 83% of global profit driven by patents for medicines was made by the pharmaceutical sector in the US alone, compared to nine other foreign markets. According to research released by Vital Transformation on EU biotech competitiveness, with a few exceptions, the US is the only viable exit route for foreign investors in biotech to sell their mid-stage IP. This explains why 70% of global mature assets in 2017 were acquired by U.S. based acquires. So, whilst it’s true that the U.S. taxpayer now pays and likely subsidises the global pharmaceutical industry, the fact is the U.S. also gains an enormous competitive advantage in having the ability to acquire and own the majority of global cutting-edge biotech and pharmaceutical innovations, and capture the late stage value creation.
You Can’t Have Your Cake and Eat it Too.
Returning to Secretary Azar’s presentation at the Brookings Institute, he also said that, “Over the next five years . . . we will go from paying 180 percent of what other countries pay for these drugs to 126 percent of what they pay. . . The pharmaceutical industry reports they spend an average of 21 percent of revenue on R&D. So at most this model could pull around $700 million out of the entire pharmaceutical industry’s annual R&D budget, which they boost is more than $70 billion a year right now. These savings, while very substantial for American patients and American taxpayers, cannot, therefore, possibly pull out more than 1 percent of R&D.”
Given Secretary Azar spent nearly a decade working for Eli Lilly, one would think that his understanding of biopharmaceutical economics and R&D would be more grounded. Regardless, we will now investigate his assertion to see both what the net impact on the individual firm will be, and how this could translate to R&D’s bottom line.
The pricing studythat Secretary Azar mentions in his presentation was performed by the consultancy IQVIA, investigating prices of the top 27 drugs by spending in the Medicare Part B database. The methodology is quite simple, in that IQVIA compares the average cost of a US drug to that of the same dose against a basket of countries in Europe and Asia.
One of the drugs listed in the IQVIA study is Tysabri, from the U.S. based company Biogen. The study shows that the US tax payer pays, per dose, nearly three times what other global regions pay on average. What would happen to Biogen’s R&D expenditures simply by reducing the cost of Tysabri to match what is paid internationally plus 26%, as is advocated under the plan announced by Secretary Azar?
According to Biogen’s 2017 annual report, sales of Tysabri represented $2 billion of their global revenue of $12 billion. In other words, roughly 17% of Biogen’s total revenue was derived from the sales of this one product in fiscal year 2017. $1.12 billion of Biogen’s revenue from Tysabri came from the U.S.; the rest of the world was responsible for roughly $860 million. While only $306 million of their US sales were accountable to Medicare PartB, there is little doubt that a forced reference price would radically impact all US prices, as any insurer would negotiate based upon the price paid by Medicare PartB.
In 2017, Biogen spent $2.26 billion on R&D. A cut of $670 million in U.S. revenue due to reference pricing equates to a whopping hit of 30% of Biogen’s total R&D budget, not 1%. Or, if Biogen were to absorb the loss of sales in Tysabri and hold the R&D budget constant, it would then impact Biogen’s free cash flow, also roughly $2 billion in 2017. The fact is if the profits are not spent on R&D, then they are reinvested in acquiring new, cutting edge companies or intellectual property – perhaps the next Biogen.
Finally, one must also keep in mind that this represents the impact of reference pricing with only one product. Many companies, Roche and J&J for example, have multiple products that have been included in the IQVIA analysis.
Reference pricing is a mandatory price ceiling that will impact those products that consume the largest portion of the current Medicare Part B Budget; these are often highly targeted and effective new therapies. Do we, as U.S. Citizens, need to have an honest discussion regarding the substantially higher prices that the U.S. consumer pays for medicines compared to those in say, Europe? Yes, absolutely. But to assume that a good solution is targeting the most successful and needed new therapies with mandated price ceilings, often for drugs coming from innovative US companies, and then state that it will only impact 1% of R&D is sky-high rhetoric untethered from reality.
In fact, the impact on R&D and innovation globally will be devastating.
The most successful drugs a company sells are those products which fund R&D and future acquisitions; i.e. the future products a company needs to make in order to stay in business are built upon the revenues of their currently successful products. This is the entire point of innovation in biopharma; 92% of all new innovations fail, success is rare, it takes a long time to make a product, and truly novel products are expensive.
Lest we forget, biotechnology and pharmaceutical patents also expire; the products IQVIA investigated took 10 years to come to market on average, and then have only 10 years of sales before the intellectual property becomes public domain and the therapies have generic competition. Targeting only the most new, successful, and cutting-edge technologies for arbitrary price ceilings will have a debilitating impact on U.S. innovation and likely drive biotech firms to move to other markets.
In my capacity as the Director of Vital Transformation, I am often invited to moderate conference panels with members of the European Commission and other officials from the EU member states. One question I often ask is, “Why hasn’t the EU created an Amgen or Gilead”? Invariably, their answers are a combination of a lack of investors with the required risk capital and the lack of a fully functioning reimbursement market; obviously, what is not stated is that the two are directly connected.
The last European company that tried to become a truly independent market leader was Tigenix, a ground-breaking stem cell company from Belgium that at one time was valued over $1 billion on the Euronext. Regulatory applications were filed for their lead product with both the European Medicines Agency (EMA) and FDA; the EMA approved their application in 2008, the FDA rejected it in 2009. Even with an EMA license, without access to the US market Tigenix only had $4 million in sales in 2013 before they withdrew their lead product.
Tigenix’s story is a cautionary tale, and one that could easily see US companies having to move to Korea or Singapore if price ceilings that radically impact an innovative company’s ability to price new products are enacted. While it is understandable that forcing a solution to high-priced medicines would be politically popular in the short term, it would behoove those in authority to heed the words of Milton Friedman who said, “When government in pursuit of good intentions tries to rearrange the economy, legislate morality, or help special interests, the costs come in inefficiency, lack of motivation, and loss of freedom. Government should be a referee, not an active player.”
Duane Schulthess is the Managing Director of Vital Transformation. His 2012 publication “Unlocking the Value of Personalised Healthcare in Europe, Breast Cancer Stratification” is considered a ground-braking analysis in the field of personalised medicine, regularly cited in presentations by the European Commission. He has a BA from the University of the Pacific where he was also nominated to the Phi Kappa Phi honour society, and an MBA with Distinction from KU Leuven’s Vlerick Management School. He was a recipient of a Leverhulme Trust Fellowship at the Royal Academy of Music in London while also studying economics at Regent’s College. He is a Senior Associate of the UK’s Royal Society of Medicine.
This article was edited to on January 4th, 2019, to clarify the opinion that all US prices for Tysabri would be impacted by a Medicare Part B reference price.