
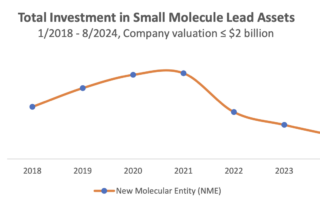
PREPRINT NEW RESEARCH: The Inflation Reduction Act’s Impact Upon Late-Stage R&D
Vital Transformation is preparing a new analysis with a total of 1148 secondary trials from 364 FDA-approved medicines, published from 2018 to 2025, obtained from Biomedtracker and clinicaltrials.gov. Using fractional multinomial logit, we model the share distribution of secondary indication studies across 19 disease groups and assess the change in this distribution post-IRA. We also assessed the number of secondary treatment studies pre- vs. post-IRA using multiple linear regression.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}